

Ca = calcium; HPT = hyperparathyroidism; P = phosphorus; PTH = parathyroid hormone.
PTH, PHOSPHORUS, AND CALCIUM
Changes in PTH, phosphorus, and calcium levels over 12 months after initiation of vitamin D and phosphate binders8*
MEAN CHANGES IN LEVELS FOR PATIENTS ON DIALYSIS RECEIVING VITAMIN D AND PHOSPHATE BINDERS*
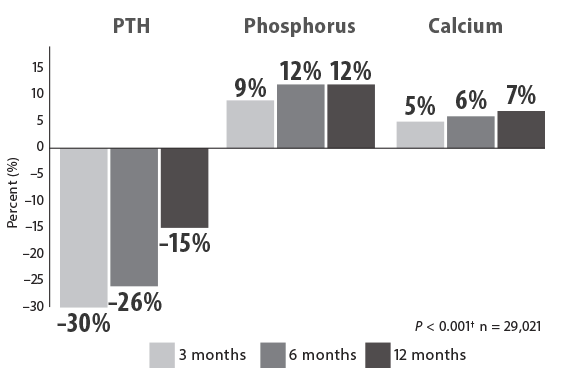
Data pooled from the database of a large dialysis provider. Total database N = 69,492 on IV vitamin D therapy, of whom 67,399 patients were prescribed either calcitriol (n = 38,378) or paricalcitol (n = 29,021). Results based on a historical cohort analysis of patients initiated on paricalcitol between 1999 and 2001. During a 12-month follow-up analysis, the mean percentage change from baseline was calculated for each patient at 3, 6, and 12 months. Target value for iPTH was < 300 pg/mL. Most patients also received phosphate binders. No specific therapies were suggested. At 3, 6, and 12 months, the mean doses of paricalcitol per administration were 4.2 μg, 4.3 μg, and 4.3 μg, respectively.8
*Results shown for patients treated with paricalcitol only.
†For each point vs baseline between groups.
INITIATION OF SECONDARY HPT THERAPIES
Increasing levels of PTH and calcium were present at the time of Sensipar® (cinacalcet) initiation9
CHART AUDIT ANALYSIS
Sensipar® End-Stage Renal Disease (ESRD) Dialysis Patient Chart Audit. Survey conducted Q2 2014. Chart audit data gathered over a period from March 24, 2014 to May 5, 2014 from 144 nephrologists and included 537 patients on dialysis. Each nephrologist provided patient information from 3–5 patients on dialysis who were diagnosed with secondary HPT. Data from a subset of nephrologists (n = 34) who were classified as having > 5% of patients initiated on Sensipar® at iPTH ≤ 500 pg/mL and who would not start a patient on Sensipar® with the following laboratory values: iPTH: 530 pg/mL, calcium: 9.6 mg/dL, phosphorus: 5.5 mg/dL are shown. N numbers for individual laboratory values varied based on availability.9
HPT = hyperparatyhroidism; iPTH = intact parathyroid hormone; PTH = parathyroid hormone.
HPT = hyperparatyhroidism; iPTH = intact parathyroid hormone; PTH = parathyroid hormone.